Ted Med - 'imagining the future of medicine'
Royal Albert Hall, London - 21/04/14 - 2-7 pm
An afternoon of lectures on numerous aspects of modern health care: The future of medicine is full of innovative ideas that are technology supported, individualised and creative.
But which ideas are feasible? What is mere fiction? And - what has already been put into practice?
But which ideas are feasible? What is mere fiction? And - what has already been put into practice?
|
Introduction
As osteopaths we are unlikely to get into the awkward situation of having to replace somebody's heart valves... But when a cardiac surgeons talks about the interrelatedness of structure and function, wouldn't that make you prick your ears? Let me introduce you to some of the more interesting ideas and concepts from this series of lectures. J. El Imad
Here we go: Top notch IT specialists working hand-in-hand with neurologist to develop smart things such as real-time EEG's, smartphone-driven pre-warning systems for epileptic sufferers etc. This is probably a prime example of how multi-disciplinary out-of-the-box thinking can lead to huge steps into a remarkably new direction... 
Us at the 'lecture' theatre.
Ali Parsa
In a similar spirit, ex-consultant Ali Parsa is working on an app enabling patients to consult GP's with a very short notice, from anywhere in the world and entirely via their phone. My thought on that: Smartphone apps are not the solution to everything, are quite impersonal and sterile and I do wonder how many of them are actually developed with the principle aim of selling them on for ridiculous amounts of money rather than Parsa's alleged motif: Innovation is not about what you can offer, but about what people need. Do we really need all this or is the problem of modern day health care one that has to be tackled on an entirely different level? Individualisation of intervention, appreciation of human values, reversly, valuing the work of carers, decreasing and controling the power of pharma companies / money, etc. And please spare me from the pathetic notion that this app is gonna improve health care in Africa! Katherine Sleeman
This afternoon at the BSO clinic a patient told me about how afraid he was of having a stroke and dying slowly rather than just passing away. This made me think of Dr Sleeman's lecture yesterday - in itself an impressive one -, but this incident highlighted to me how relevant her topic is: Death and dying. We never speak about Death. In a hospital context, that is probably more relevant than to osteopaths, but in general society can be seen to have a huge deficit here: Why not prepare death in a way that helps everybody affected? Why not call the child by its name and do something not against dying, but for a healthy way of dying? A terribly interesting research finding about palliative care: Terminally ill cancer patients (Note my choice of words! I meant: People that are going to die, soon!) were allocated to cancer care and cancer care plus palliative care. The latter group not only had less symptoms, shorter hospital stays, and better psychological values - they also lived longer! Of course 'being cared for' does not decrease you life span. It's not a trade off between intervention and a better life; It's more quality and more quantity of life. Why is that not accepted as the right and only way to go? Because we don't talk about it... |
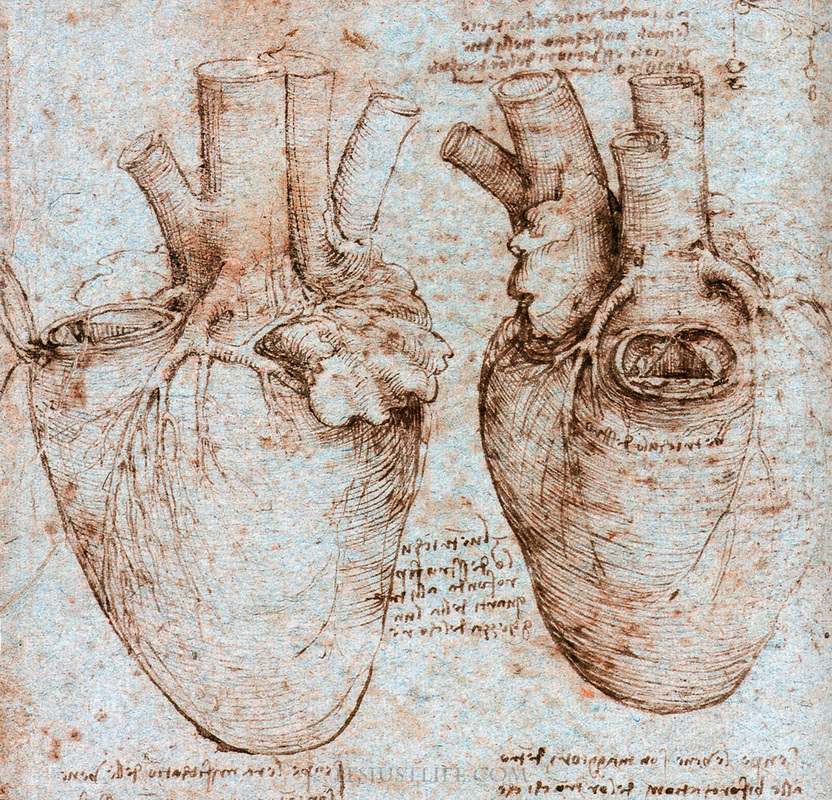
Dr Francis Wells
This is the cardiologist I already mentioned. He managed to deduce an fundamental functional concept regarding the aortic valves from 16th century drawings of Da Vinci: It is not the actual back-flow from the aorta that pushes the valve shut; It is the fluid vortices resulting from the actual outflow from a large space (ventricle) through a small whole into a larger space of less fluid (the aorta itself). These vortices open the individual flaps of the valve so that they are already almost shut when back-flow actually occurs on relaxation of the ventricle. Dr Wells spoke about a few fundamental principles according to which examine nature: First, ask the right questions: 'Why' more than 'What' or 'How'. Look and See: Look at things for what they really are not just at what they look like. And finally: Form and Function, or as Darcy W. Thomson said: Shapes in nature are a representation of the forces acting on them. With these principles in mind, Dr Wells contributed significantly to improved prostheses and methods of valve repair and replacement. Tali Sharot
Another neuroscientist, Sharot's research has fundamental implication for osteopathic practice, too: How do you get people to do things that are good for them / abstain from things that are bad. Point 1: Not with threats. Point 2: Positive language and motivation in the true sense of the word. As such, the following three concepts seem to work independent of age and gender: - immediate rewards - social integration - progress. As an example, nurses and doctors on a hospital ward could be made to sterilise their hands when entering a treatment room with a compliance rate of 90% (compared to an initial 1%) by implementing a simple system: Every time someone complied with the demand to wash their hands, a LED-display lighted up with a positive message (imm. reward). The whole ward worked together (social aspect) to achieve a goal (progress). Ever tried to make a patient do his exercises by telling them about how disabled they will be in two years time if they don't? Rethink! Ben Goldacre on 'Bad Science' - his aim: make any researcher disclose all methods and results of all of their trials, not just the one which produced positive results or results in the interest of the pharma company.
An old (and much better) TED talk by him (than the one we saw yesterday): |
